
Hand and finger injuries are very common injuries. Hands are involved in most of our daily activities and are prone to a number of injuries, such as cuts, burns, sprains, broken or sprained fingers, tendon injuries, etc. In this article, we will talk about some of the most common hand and finger injuries, as well as their immediate and definitive treatment.
Table of contents
Anatomy
The anatomy of the hand is complex. Each hand consists of 27 bones, including 8 wrist bones, 5 metacarpals and 14 finger bones, or phalanges. If we consider the other structures involved in the anatomy of the hand (nerves, vessels, muscles, tendons, ligaments, etc.), we realize that injuries to the hand can lead to a wide variety of problems.
The fingers, from the index finger to the little finger, have 3 phalanges each (proximal, middle and distal), and three joints: the distal and proximal interphalangeal joints (DIP & PIP), as well as the metacarpophalangeal joint (MCP).
The thumb has two phalanges & two joints, the interphalangeal and the metacarpophalangeal joint. The joints are held together by collateral ligaments and the volar plate.

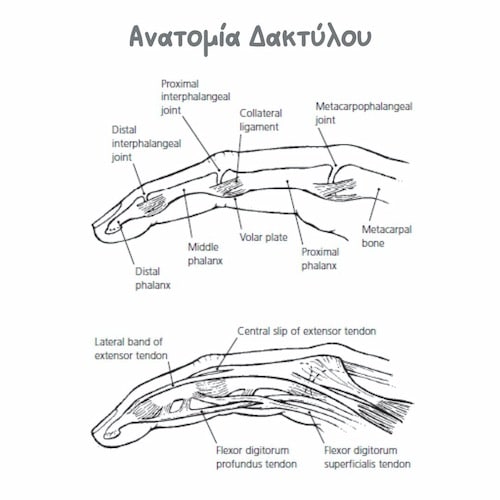
Fingers move with the help of tendons. On the dorsal surface of the hand are the extensor tendons. Each extensor consists of a central slip, which lodges in the middle phalanx and extends the PIP, and two lateral bands, which terminate in the terminal phalanx and extend the DIP. On the palmar surface of the fingers are the flexors. The flexors include the flexor digitorum superficialis (FDS), and the flexor digitorum profundus, or FDP. The FDS terminates on the middle phalanx and is responsible for flexion of the PIP, while the FDP terminates on the terminal phalanx and performs flexion of the DIP.
Mallet finger
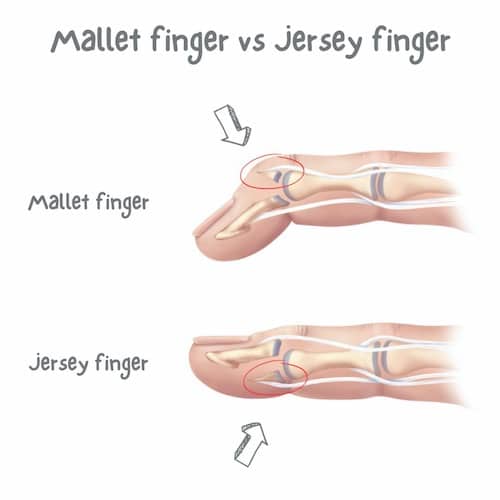
Mallet finger is the name given to the deformity of the finger that includes inability to extend the terminal phalanx (and the DIP joint). Mallet finger is due to a transection, or tear of the extensor tendon. Often, the disruption of the extensor mechanism can also involve a small piece of bone (bony mallet finger).

This injury is particularly common, with a typical mechanism being a direct blow on the bent terminal phalanx, during work, sports or daily activities. It is not uncommon to see a basketball player, for example, with multiple malformed fingers (multiple mallet fingers). Many times, the patient considers the injury to be trivial or less important, resulting in a delayed visit to the specialist.
The treatment is in most cases conservative, with the use of a special splint for 6-8 weeks. The splint keeps the DIP in extension 24 hours a day, but must allow free movement of the PIP. Surgery is required in case of transection of the tendon from an open wound, joint involvement >50%, or in any case where the joint is subluxed. The surgery can also be done under local anesthesia and usually includes either extension block pinning with needles, or fixation with a small screw, if the bone fragment is large enough.
Jersey finger
The rupture of the deep flexor (FDP) in the so-called zone I, i.e. its detachment from the distal phalanx, is also known as Jersey finger. The injury often occurs in athletes when the finger "hits" a teammate's uniform, and is subjected to a sudden force of extension while in flexion. The ring finger is the most commonly involved finger.
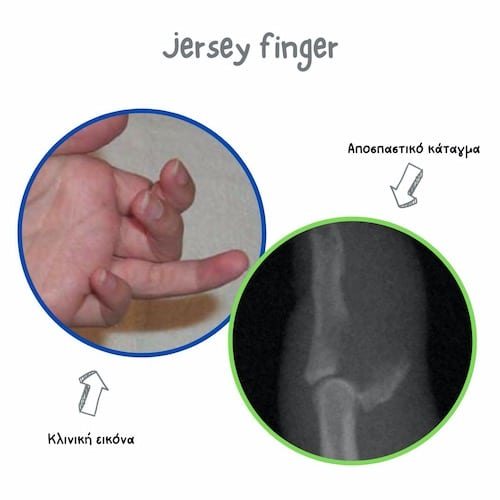
The patient usually presents with an inability to actively flex the DIP. Treatment is usually surgical, with repair of the tendon in its anatomical position. It is not uncommon for the tendon stump to move more centrally, requiring a second palmar incision to locate it. If the patient presents late, a 2-stage tendon reconstruction, or other techniques, may be needed.
Boutonniere deformity
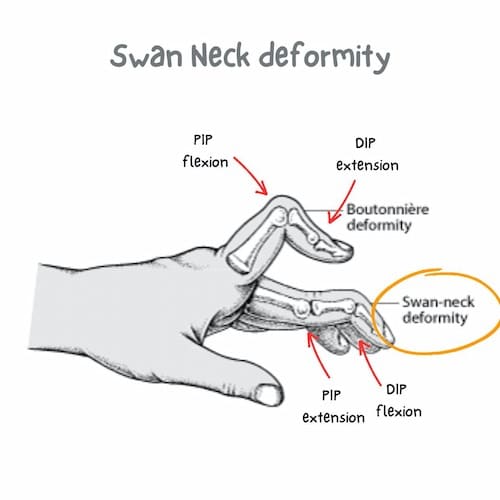
The Boutonniere deformity is due to a rupture of the central bundle of the extensor mechanism of the finger from its insertion in the middle phalanx. Diagnosis is easily made clinically by the characteristic deformity, which includes PIP flexion & DIP extension, or by clinical tests, such as the Elson test.
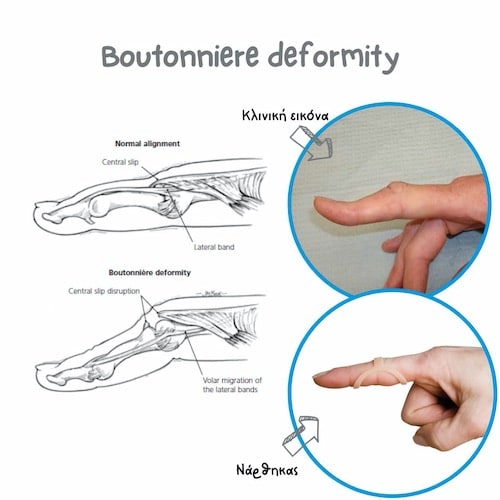
The rupture is usually traumatic, but the deformity can also be due to chronic diseases. Typically, patients with rheumatoid arthritis develop a Boutonniere on at least one finger in up to 50% of cases. The lesion is pliable in the initial stages, but over time can become rigid if neglected.
Treatment is usually conservative in acute cases (<4 weeks) without an open wound, with a splint that maintains the PIP in extension for 6 weeks, with partial use of the splint at night or during activities for another 4-6 weeks. Open cuts or a fracture with a displaced bone fragment require surgery. Neglected cases with stiffness and degenerative deformity in the context of systemic disease require a more specialized surgery.
Swan neck deformity
Swan Neck differs from Boutonniere in that it exhibits extension of the PIP and flexion of the DIP. Although it can be the result of trauma, it usually occurs as a degenerative deformity in patients with rheumatoid arthritis (50%). The main causative factor is laxity of the volar plate.
Traumatically, a neglected mallet finger, or flexor superficialis tear may contribute. Minor deformities can be treated conservatively, with splints. In more rigid or chronic forms, surgical correction is required (eg, volar plate advancement +/- central slip tenotomy).
Skier’s thumb
The ulnar collateral ligament or UCL of the thumb is a strong ligament located at the base of the thumb, in the web space between the thumb and the index finger. The UCL can get sprained or torn when your thumb is forced away from your hand, i.e., when hit by a ball or while skiing. An acute UCL injury is common in sports, including skiing, football, volleyball, and is often referred to as skier’s thumb. A chronic variety of the injury, known as gamekeeper’s thumb, is caused by attenuation of the UCL due to repeated stress.

An overstretched or partially torn ligament, as determined by clinical exam or MRI, can be treated conservatively with a splint. The splint must be worn for about 6 weeks to give your ligament the chance to heal properly. However, a fully torn ligament usually needs surgery. That’s because the UCL usually gets displaced away from its insertion and another structure called adductor aponeurosis gets interposed, preventing the UCL from healing in its anatomical position (Stener lesion). If the UCL tear is caught early, it can be repaired with a special device called a suture anchor.
Boxer’s fracture
The most common metacarpal fracture is the fracture of the neck of the 5th metacarpal, also known as a boxer's fracture, from the classic mechanism of the punch that breaks its target. This fracture usually occurs after a blow of the closed fist on a hard surface (eg, a wall), but it can also occur from other injuries (eg, sports or a car accident). The distal part of the fracture is usually displaced palmarly.
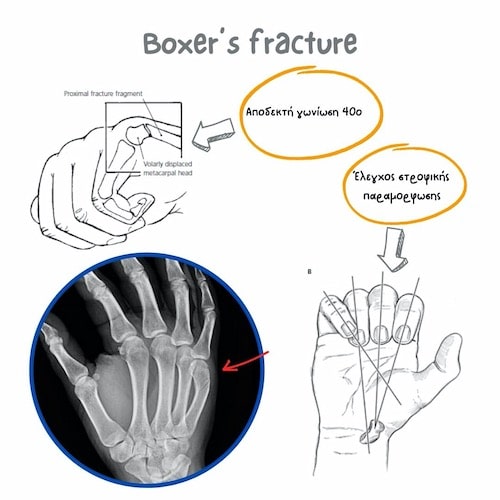
The fracture should be checked clinically and radiologically. Since the accepted angulation in 5th metacarpal fractures is 40°, most fractures of this type are treated conservatively. Larger angulations can be retracted closed, under local anesthesia. The most critical, perhaps, factor that can lead to the decision for surgical treatment, is the possible malrotation of the finger. If the finger has rotational deformity, then surgery is necessary.
Thumb fractures - Bennett & Rolando
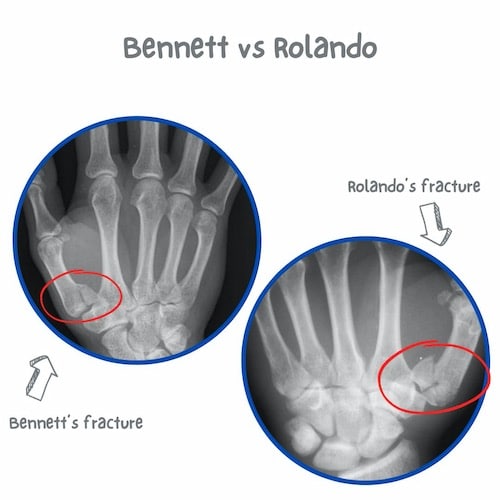
A Bennett fracture is an intra-articular, oblique fracture of the base of the 1th metacarpal. The Rolando fracture is a similar but more complex fracture, with greater comminution. It is important that these fractures are recognized in time, due to their instability and the need for anatomical reduction and osteosynthesis. If a Bennett fracture heals with persistent displacement, the patient is prone to stiffness, pain, or instability in the short term, as well as arthritis in the long term (within 5-7 years).
Finger fractures
Finger fractures are common, and may involve the distal, middle, or central phalanx. The mechanism may include some sports or professional activity, falls, etc. The distal phalanx and the little finger are most often involved. The diagnosis can be easily made with simple x-rays. Treatment can be conservative or surgical, depending on the complexity of the fracture, possible intra-articular involvement, dislocation, rotational deformity of the finger, etc.
Finger dislocations
Another finger injury is dislocations, which can involve the distal phalangeal (DIP), proximal (PIP), or metacarpophalangeal (MCP) joint. PIP is most often involved. In any case, a fracture may be present. PIP dislocation is most often dorsal. The reduction can most often be done closed under local anesthesia. If closed reduction fails, then open reduction is needed due to soft tissue involvement.
Ring avulsion injuries
A ring avulsion injury can be a potentially serious injury to the hand and can threaten the viability of the finger. The usual mechanism is a sudden engagement of the ring finger (ring finger) on a fixed object, resulting in sudden traction and circular injury to the soft tissues of the finger. The degree of vascular damage under the skin can vary and be worse than apparent. The injury requires immediate treatment by a specialist surgeon due to the immediate risk of losing the finger. In 2015, comedian Jimmy Fallon, almost lost his finger due to a similar accident.
Nailbed injuries
The nail phalanx is often injured. Fractures are common and may be open, i.e. with overlying trauma. Also common is subungual hematoma, which may sometimes require needle drainage. In children, Seymour fractures are common, i.e. displaced fractures of the terminal phalanx of the finger, with accompanying nail bed injury. Treatment involves reduction of the fracture and suture repair of the subungual region.
If you suffer from a finger injury, you should seek expert care. Dr Panagopoulos will evaluate your condition and offer appropriate treatment to restore your function and relieve your pain.
What's the difference between mallet finger & jersey finger?
Mallet finger involves the extensor tendon, whereas jersey finger involves the flexor.
What's the difference between mallet finger & boutonniere deformity?
Mallet finger involves the insertion of the extensor tendon to the distal phalanx, whereas boutonniere's involves the insertion of the central slip to the middle phalanx.
Find us
Book an appointment with us today