Georgios Panagopoulos MD | Orthopaedic Surgeon
TFCC Tear

Η ρήξη τρίγωνου χόνδρου ή ρήξη TFCC (Triangular Fibrocartilage Complex) είναι η μερική ή πλήρης βλάβη του τριγωνικού ινοχόνδρινου συμπλέγματος του καρπού, μιας σύνθετης ανατομικής δομής στην ωλένια πλευρά του καρπού που λειτουργεί ως κύριος σταθεροποιητής της κάτω κερκιδοωλένιας άρθρωσης και ως αποσβεστήρας φορτίων μεταξύ ωλένης και καρπικών οστών, προκαλώντας πόνο, αστάθεια και λειτουργικό περιορισμό του άνω άκρου.
Key takeaways at a glance
What's a TFCC tear?
A TFCC tear is a common cause of ulnar-sided wrist pain, especially after trauma or repetitive loading.
Is diagnosis difficult?
It is frequently misdiagnosed or mistaken for tendinitis or a minor wrist injury.
What's the typical mechanism of injury?
TFCC tears can be traumatic or degenerative.
How is it diagnosed?
MRI and wrist arthroscopy play a critical role in diagnosis.
What's the treatment?
Many TFCC tears respond to conservative treatment, but selected cases require arthroscopic surgical repair.
Is timely diagnosis important?
Accurate diagnosis is essential to prevent chronic pain and wrist instability.
Table of contents
What Is the TFCC?
The Triangular Fibrocartilage Complex (TFCC) is a complex anatomical structure located on the ulnar side of the wrist.
It consists of:
- a fibrocartilaginous disc
- ligaments
- tendon components
- capsular structures
Its main functions are:
- stabilization of the distal radioulnar joint (DRUJ)
- load transmission between the ulna and carpal bones
- contribution to grip strength and forearm rotation
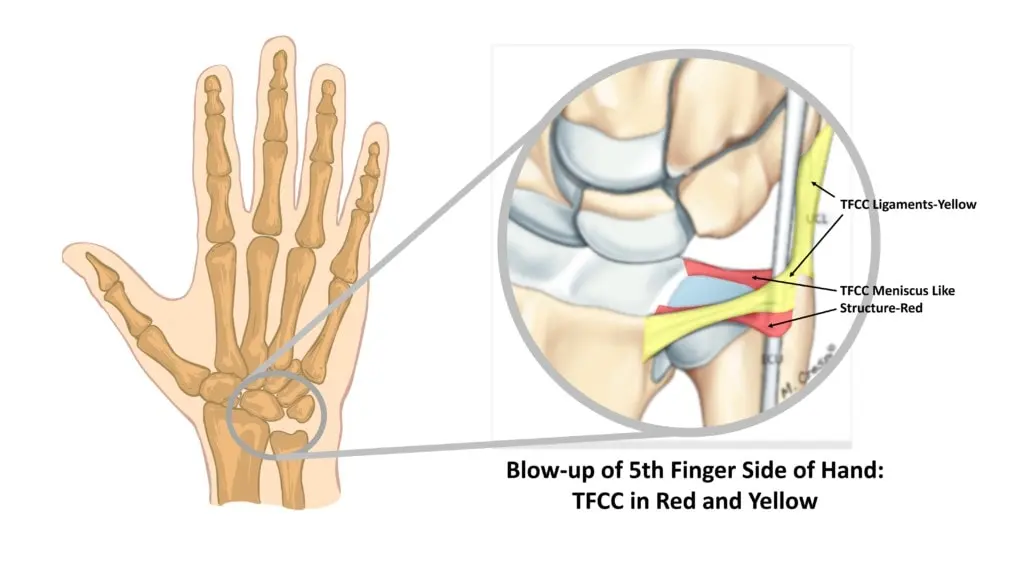
More specifically, the triangular fibrocartilage complex consists of the following delicate anatomical structures:
- fibro-cartilaginous disc
- ulno-meniscal homologue
- dorsal and volar radio-ulnar ligaments
- ulnar collateral ligament
- extensor carpi ulnaris (ECU) tendon sub-sheath
The TFCC is a key stabilizing structure essential for normal wrist biomechanics.
What's a TFCC tear?
A TFCC tear is a partial or complete injury to one or more components of the triangular fibrocartilage complex, leading to:
- wrist pain
- instability
- wrist weakness
It is one of the most common causes of chronic ulnar-sided wrist pain.
In general, tears are also divided into central tears & peripheral tears. The topography of the tears affects the final treatment.
How is it caused?
🔹 Traumatic tears
Typically occur after:
- a fall on an outstretched hand
- sudden twisting of the wrist
- sports injuries (tennis, golf, CrossFit)
- work-related accidents
🔹 Degenerative tears
Associated with:
- age
- repetitive wrist loading
- positive ulnar variance
The difference in length between the radius and ulna, with the ulna being more often longer (positive ulnar variance), is also considered a predisposing factor for the occurrence of triangular cartilage tears.
The study of the blood supply of the triangular cartilage has shown that only 15%-20% is well vascularized, with the remaining portion being avascular, resulting in increased difficulty in healing, especially in central tears, i.e. those that are close to the radius.
Degenerative TFCC tears may represent progressive wear rather than a single traumatic event.
Symptoms
Symptoms may be acute or insidious and include:
- Pain on the ulnar side of the wrist
- Pain during forearm rotation (pronation–supination)
- Clicking, catching, or popping sensations
- Weak grip strength
- Worsening pain with loading or weight-bearing on the wrist
Ulnar-sided wrist pain should always raise suspicion of a TFCC injury.
Traumatic vs Degenerative Tears
Distinguishing between these two entities is clinically crucial:
| Traumatic TFCC Tear | Degenerative TFCC Tear |
|---|---|
| Younger patients | Older patients |
| Sudden onset | Gradual onset |
| Better healing potential | Often associated with arthritis |
Tears of the triangular cartilage are divided into traumatic and degenerative, i.e. the result of wear and tear over time. Traumatic tears are due to direct injury to the wrist and occur mainly in young people, who usually have significant sports activity. Degenerative tears appear after the age of 40, without a clear history of injury.
Diagnosis
Clinical exam
Diagnosis begins with a medical history and physical examination to assess range of motion, stability, and the presence of tenderness in the wrist. Plain radiographs are usually not diagnostic, and MRI is required to confirm the clinical diagnosis. In questionable cases, diagnostic arthroscopy may be required.
- Localized tenderness on the ulnar side
- Positive provocative tests (e.g., ulnar fovea sign, ballotment, piano key sign)
- Assessment of DRUJ stability
The pain is typically localized over the distal end of the ulna, in the area of the triangular cartilage (fovea sign). It is reproduced in extreme positions of wrist rotation. The reproduction of pain in ulnar deviation is characteristic, as is the piano key sign, where reciprocating pressure on the distal end of the ulna reproduces the symptom. Comparison with the contralateral healthy wrist is of utmost importance.
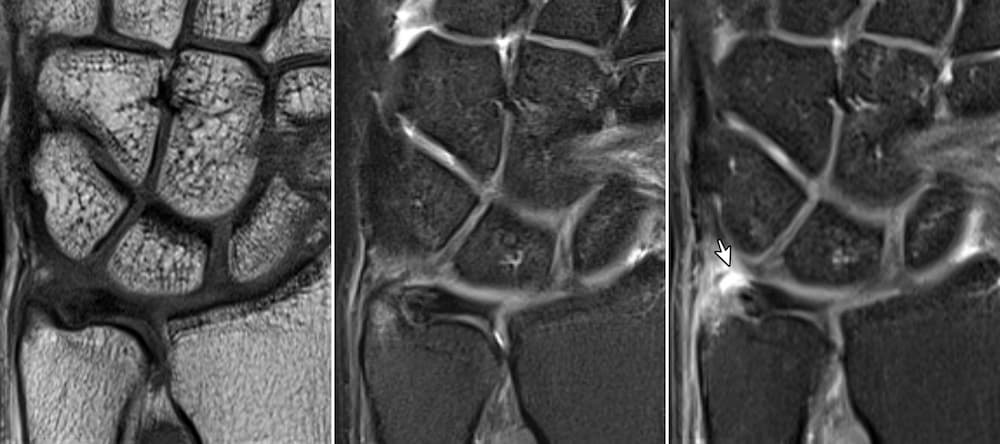
Imaging
- MRI of the wrist: primary imaging modality
- MR arthrogram: increased sensitivity in selected cases
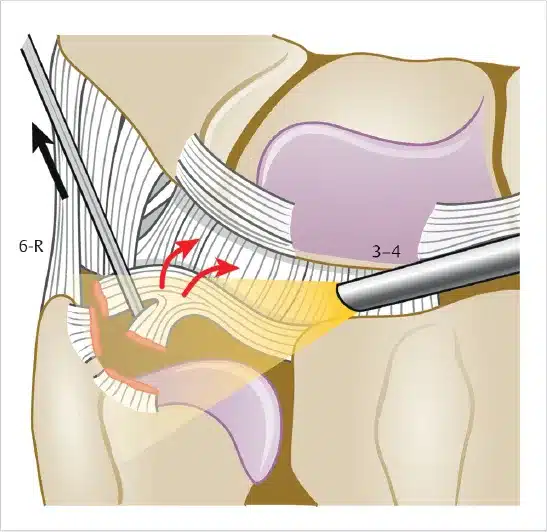
Wrist Arthroscopy
- Considered the gold standard
- Allows simultaneous diagnosis and treatment
Wrist arthroscopy remains the most accurate diagnostic tool for TFCC pathology.
Treatment of TFCC Tears
Conservative treatment
Indicated in:
- stable tears
- mild to moderate symptoms
- degenerative lesions without instability
Includes:
- immobilisation
- NSAIDS
- physiotherapy
- activity modification
⚠️ Persistent symptoms require reassessment.
Surgical treatment
Surgical treatment is considered when:
- symptoms persist despite conservative management
- distal radioulnar joint instability is present
- he patient has high functional demands
Wrist arthroscopy may entail:
- debridement
- repair
- reattachment
Arthroscopic management of TFCC tears is minimally invasive and has great functional outcomes.
🔧 When Is Surgery Indicated?
Surgical treatment is considered when:
- symptoms persist despite conservative management
- distal radioulnar joint instability is present
- he patient has high functional demands
- a traumatic tear occurs in a young, active individual
- anatomical factors contribute to ongoing TFCC overload
The decision for surgery is guided primarily by symptoms and functional limitation, not imaging alone.
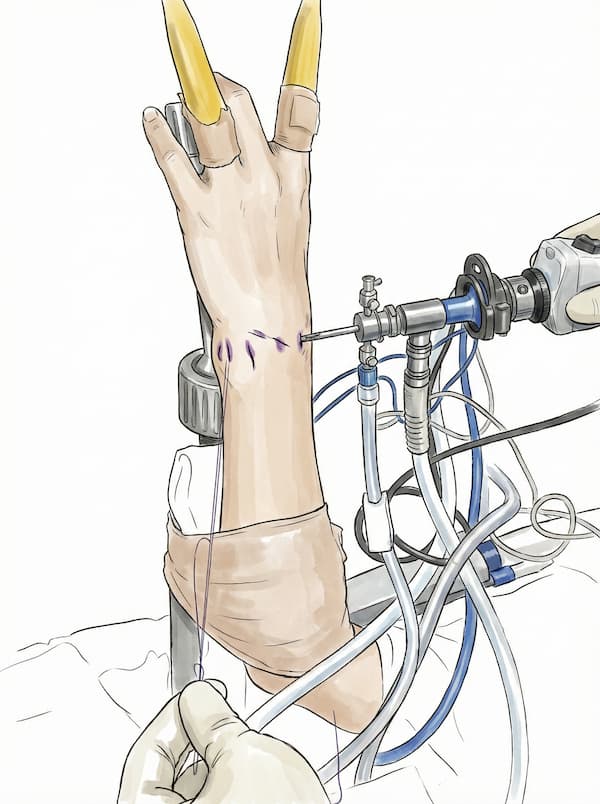
Wrist Arthroscopy – Treatment of Choice
Wrist arthroscopy is the preferred surgical technique for most TFCC tears.
It is:
- minimally invasive
- performed through small portals
- highly accurate
- associated with faster recovery
Arthroscopy allows direct visualization of the TFCC and precise treatment of the lesion.
Types of Arthroscopic TFCC Procedures
🔹 Arthroscopic Debridement
Best suited for:
- degenerative tears
- central TFCC lesions
- stable distal radioulnar joint
Goals:
- removal of damaged tissue
- pain relief
- improved wrist motion
🔹 Arthroscopic TFCC Repair
Indicated when:
- the tear involves the peripheral vascular zone
- distal radioulnar joint instability is present
- the tear is traumatic
Advantages:
- preservation of native anatomy
- restoration of stability
- superior long-term outcomes
Peripheral TFCC tears have excellent healing potential when repaired early.
🔹 TFCC Reattachment
In selected cases, the TFCC must be:
- reattached to the ulna
- stabilized using sutures or anchors
This technique aims to:
- restore distal radioulnar joint stability
- eliminate the sensation of wrist looseness
When Are Additional Procedures Required?
🦴 Ulnar Shortening Osteotomy
In patients with:
- positive ulnar variance
- degenerative TFCC tears
- chronic ulnar-sided wrist pain
arthroscopy alone may be insufficient.
Ulnar shortening osteotomy:
- unloads the TFCC
- restores wrist biomechanics
- improves long-term outcomes
Failure to address ulnar variance may result in persistent symptoms despite TFCC repair.
🔹 Combined Procedures
In selected patients, TFCC surgery may be combined with:
- treatment of associated ligament injuries
- management of chondral damage
- correction of wrist instability
Postoperative Rehabilitation
- Short period of immobilization (procedure-dependent)
- Gradual restoration of motion
- Return to work: 4–6 weeks
- Athletes: individualized return-to-sport protocol
Early diagnosis is very important for a great outcome.
Postoperatively, immobilization of the wrist is applied for a period of 4-6 weeks and then a rehabilitation program is followed to restore wrist movement. Return to demanding sports activities is generally allowed in 4-6 months, but is individualized on a case-by-case basis.
Factors Affecting Outcome
- Type of TFCC tear
- Timing of surgery
- Appropriate surgical technique
- Compliance with rehabilitation
Successful TFCC treatment depends on accurate diagnosis and individualized surgical planning.
Key Facts – TFCC tears
- 🖐 Common cause of ulnar-sided wrist pain
- 🧠 Frequently overlooked or misdiagnosed
- 🧲 MRI helpful but not definitive
- 🔍 Arthroscopy is the diagnostic gold standard
- 🔧 Arthroscopic treatment yields high success rates
FAQs - Frequently Asked Questions
Is a TFCC tear a serious injury?
It can become serious if left untreated.
Does it always require surgery?
No. Many tears respond well to conservative treatment.
Can I continue sports with a TFCC tear?
Not without proper evaluation — continued loading may worsen the injury.
How long does recovery take?
Usually several weeks, depending on treatment type.
Find us
Book an appointment with us today