Georgios Panagopoulos MD | Orthopaedic Surgeon

Table of contents
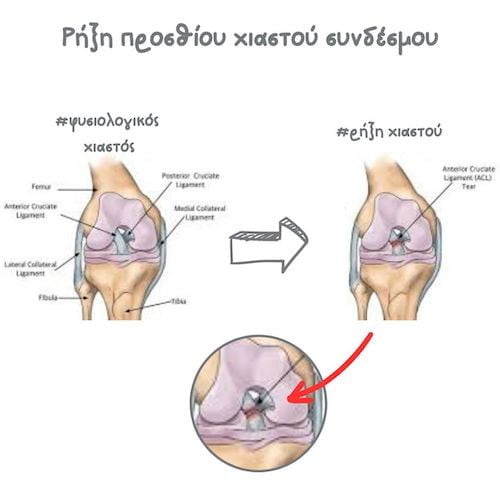
What is the ACL?
The ACL or anterior cruciate ligament is one of the most important knee ligaments and is located in the center of the knee. Its main function is to maintain knee stability and prevent the tibia (leg bone) from moving forwards. An ACL tear is one of the most common knee injuries. It also manifests frequently in association with other injuries, such as MCL tears, a torn lateral meniscus, or a PLC (posterolateral corner) injury.
What causes an ACL injury?
ACL injuries are very common in sports that require a sudden “start-stop” or a sudden change of direction, pivoting or jumping. These sports include football, basketball, skiing, squash, etc. The mechanism of injury typically includes an external twisting motion in a bent and loaded knee. You can have this if you get tackled, stop suddenly from running or land awkwardly after a jump.

What are the symptoms?
When the ACL tears, patients typically feel severe pain accompanied by a snap or pop, and the knee gives way and feels unstable. The knee also becomes very swollen very quickly. Patients are usually unable to weight bear immediately after the injury.
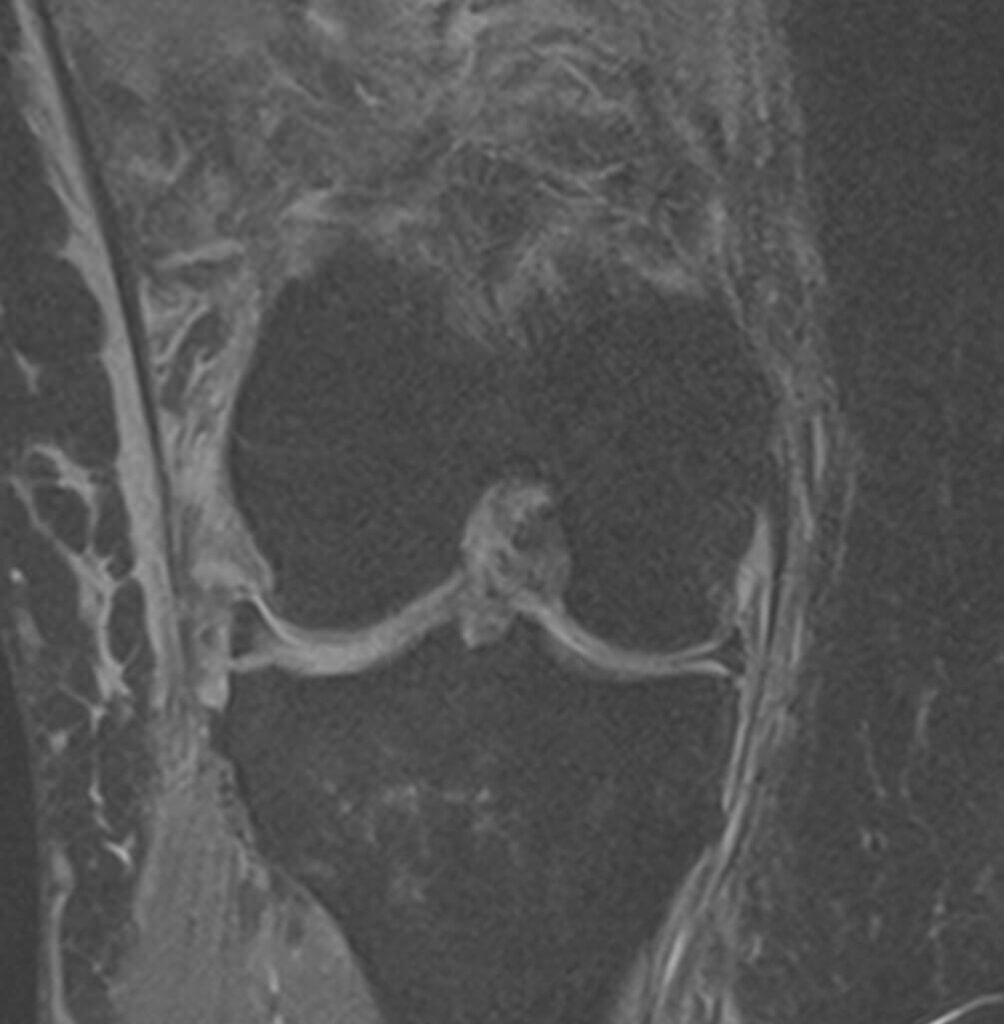
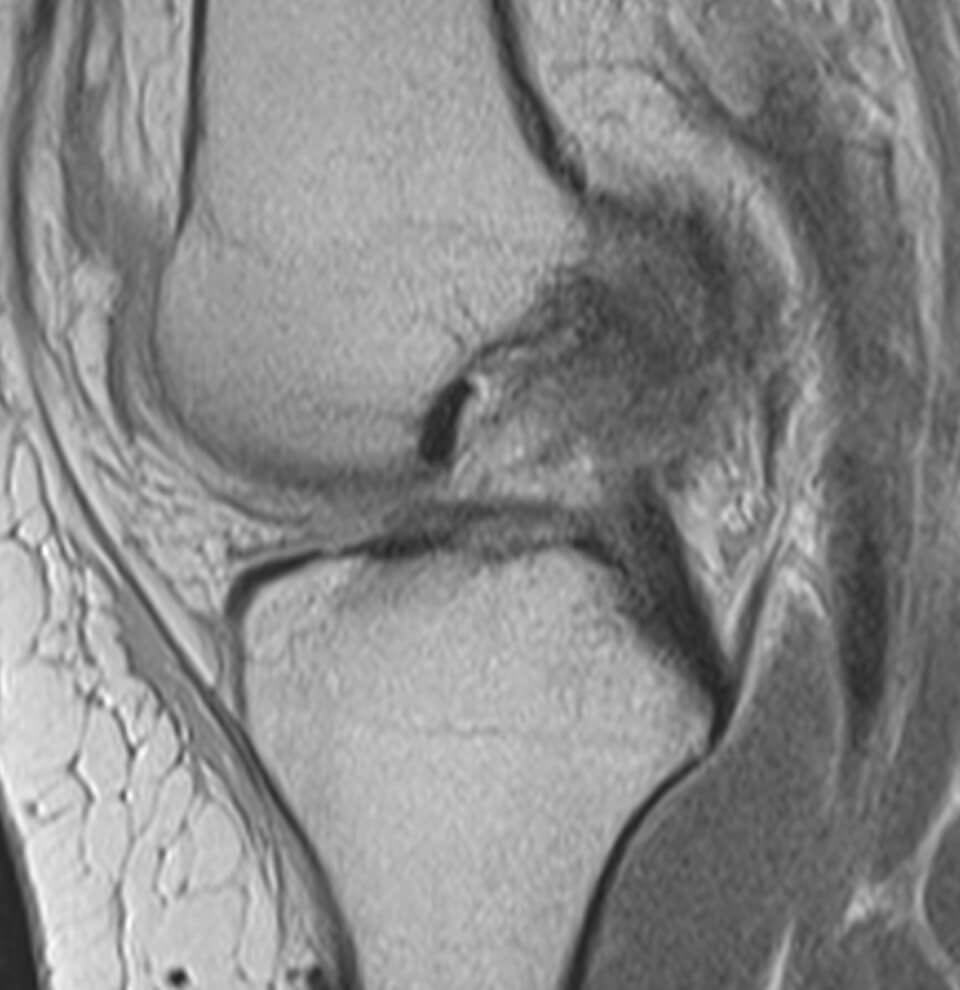
Diagnosis
History and physical exam are always important. Your surgeon may request an x-ray to rule out any associated injuries, such as broken bones. An MRI scan is always warranted to confirm a suspected ACL tear. It is always necessary to diagnose associated injuries, such as meniscal injuries, MCL tears or PLC tears.
Conservative treatment
Initial management typically involves rest, ice, anti-inflammatory medications and physiotherapy. Up to 1/3 of patients will be ok with this treatment, eventually strengthen their muscles and circumvent the ACL-deficient, potentially more unstable knee. Some patients will do initially well, but will be unable to resume sport activities to the pre-injury level and eventually might need surgery. The decision in that case boils down to their athletic aspirations. Some other patients will have a persistently wabbly knee and will need surgery.
Surgical Treatment
If the ACL injury is caught very early (within 48 hours), it may be possible to go right into surgery and have an acute ACL reconstruction. This is typically the case in high demand professional athletes for whom return to play is essential. After this time has elapsed, ACL reconstruction is usually deferred, as there is a high risk of the knee becoming super stiff (developing arthrofibrosis). For this reason, it is preferable to start physiotherapy instead (prehab), and to wait and see how the knee feels after 6 weeks. A determination can be made at that time as to whether one can let things stand or may proceed with ACL reconstruction. In the young, it is usually preferable to reconstruct the ACL, as ACL deficiency can predispose to early knee arthritis. The discussion changes when one considers associated injuries. An ACL injury associated with a lateral meniscal tear, or a posterolateral corner injury is more likely to need knee arthroscopy. MCL tears, however, usually heal nicely with conservative treatment. Another type of condition is the ACL avulsion injury. This is more common in children and warrants arthroscopic treatment early on, because if left alone the ACL will retract and become non-functional.
Knee arthroscopy may last from 20 minutes to 2 hours, depending on the complexity of the case. The surgeon will make a small incision (4mm) in the front of your knee and insert a small camera, called arthroscope, which will project images of your knee joint in a video screen. The arthroscope is essentially a slim telescope (4.5mm or 2.9mm) with a high-definition camera, surrounded by a fiber-optic tube that functions as a light source.
The surgeon will make one or two more small incisions in the front of your knee to insert tiny instruments in order to address all pathology found. Multiple arthroscopic instruments may be used during the procedure. These include probes, graspers, punches, rasps, elevators and suture cutters. Power instruments, such as shavers, or radiofrequency probes may also be used.
ACL reconstruction is a very successful operation. The procedure is done under general anaesthetic and is performed for the greatest part arthroscopically. A graft is taken from elsewhere in your knee to replace your torn ACL. The most common grafts are the hamstrings, quadriceps or the patellar tendon. A tunnel is drilled in the tibia and another tunnel is drilled in the femur to accommodate the graft, which is then secured with a metal button and a screw.
Rehabilitation after an ACL reconstruction is extremely important, if not as crucial as the operation itself. Patients are encouraged to walk with walking aids and start physiotherapy as soon as possible with the aim to return to sports within 6-9 months. Satisfaction rates are as high as 90-95%.
ACL reconstruction patient-reported outcomes are excellent.
What is the cost of the procedure?
The final cost of the procedure depends on many factors, but is reasonable. Please contact us for more information.
FAQs - Frequently Asked Questions
What is the ACL?
The ACL or anterior cruciate ligament is one of the most important knee ligaments and is located in the center of the knee. Its main function is to maintain knee stability and prevent the tibia (leg bone) from moving forwards.
What causes an ACL injury?
The mechanism of injury typically includes an external twisting motion in a bent and loaded knee.
What are the symptoms?
When the ACL tears, patients typically feel severe pain accompanied by a snap or pop, and the knee gives way and feels unstable. The knee also becomes very swollen very quickly. Patients are usually unable to weight bear immediately after the injury.
How is diagnosis made?
– History & clinical exam
– X-rays
– MRI
Is conservative treatment acceptable?
Initial management typically involves rest, ice, anti-inflammatory medications and physiotherapy. Up to 1/3 of patients will be ok with this treatment, eventually strengthen their muscles and circumvent the ACL-deficient, potentially more unstable knee. Some patients will do initially well, but will be unable to resume sport activities to the pre-injury level and eventually might need surgery. The decision in that case boils down to their athletic aspirations. Some other patients will have a persistently wabbly knee and will need surgery.
When do I need surgery?
– Younger patients
– Patients with higher functional demands
– Patients who fail conservative treatment
What does surgery involve?
Surgery involves arthroscopic ACL reconstruction with an autograft.
Find us
Book an appointment with us today